Delivering High-Impact Patient Care: A Structured Medication Reviews Case Study
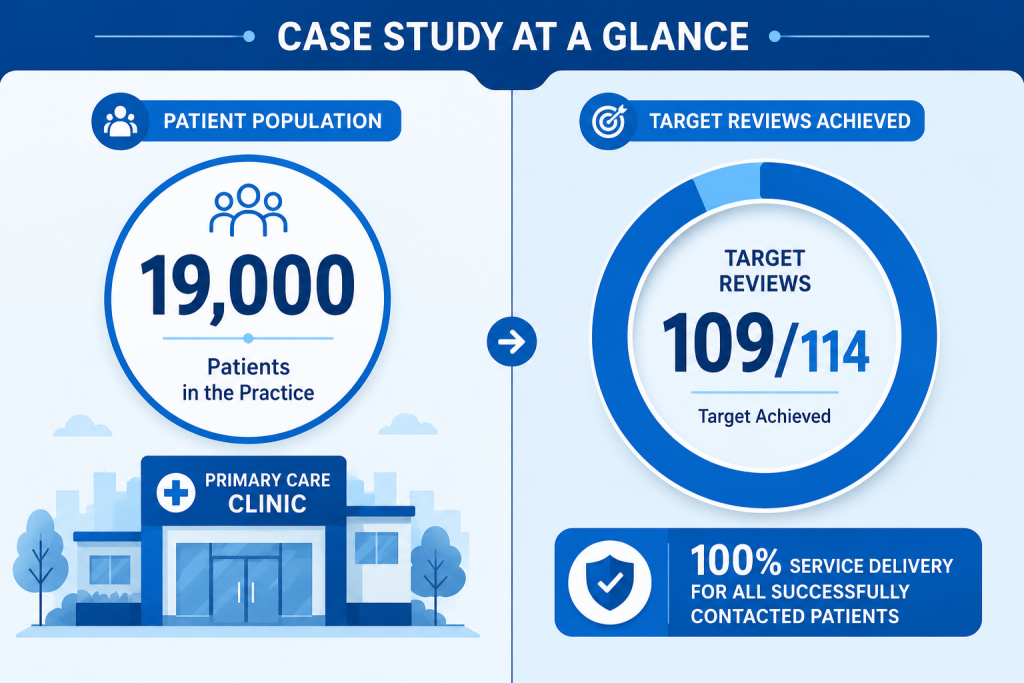
Managing clinical care effectively inside an exceptionally busy general practice requires a delicate balance between administrative efficiency and thorough clinical governance. For large primary care sites, finding the capacity to conduct deep-dive clinical assessments can challenge even the most organized leadership teams. This Structured Medication Reviews case study highlights Elm Tree Practice, a facility managing a substantial patient list size of 19,000.
Faced with the requirement to complete 114 urgent reviews, the practice chose to reject superficial “tick-box” compliance. Instead, they sought a framework that prioritized cardiovascular risk management primary care pathways and meaningful clinical interventions. By collaborating with a dedicated external pharmacy infrastructure, the practice completed 109 comprehensive reviews, achieved 100% service delivery on contacted patients, and documented 171 separate medicines optimization interventions without adding a single task to their internal administrative team.
- Scale & Efficiency: A busy practice with 19,000 patients completed 109 out of 114 targeted complex reviews with zero internal administrative burden.
- Clinical Excellence over Box-Ticking: Focused heavily on cardiovascular risk management (CVRM) to deliver 171 distinct medicines optimization interventions.
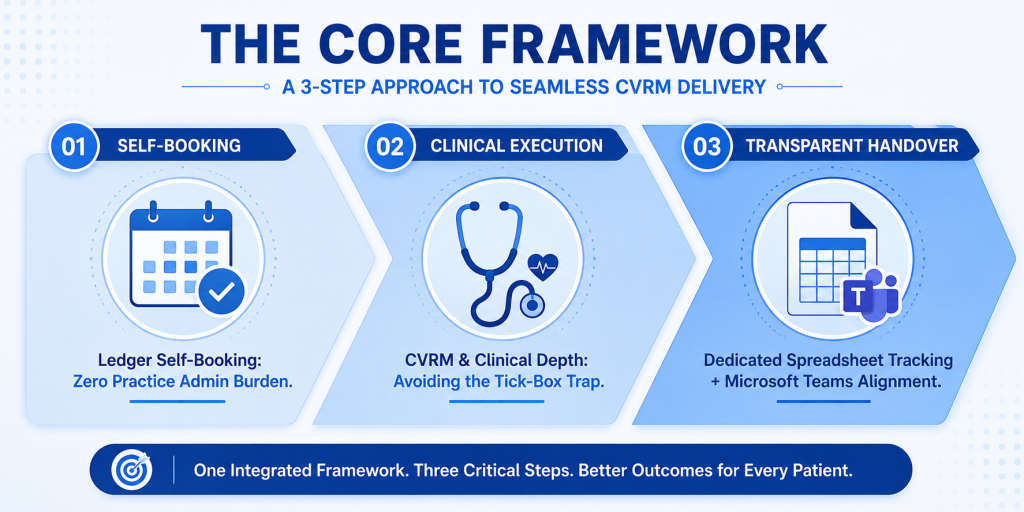
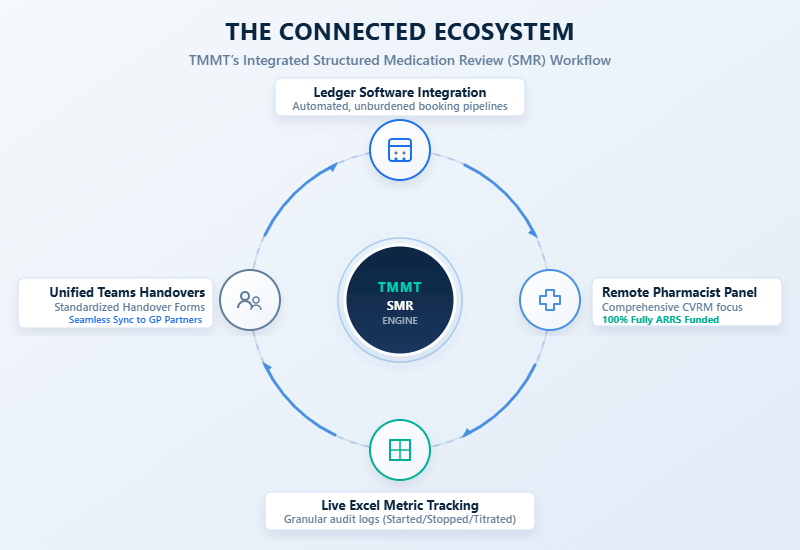
- Zero Administration Friction: Patient scheduling was fully managed externally via self-booking software (Ledger), protecting internal practice capacity.
- Meticulous Data Tracking: Leveraged parallel tracking mechanisms to capture specific medication changes (started, stopped, reduced, titrated) for transparent audit trails.
Key Learning Points
When implementing large-scale clinical audit programmes, structural setup dictates clinical outcomes. The operational strategy used in this project yielded several critical insights for modern primary care networks:
- Separation of Admin and Clinical Workflows: Moving booking management entirely outside the practice walls preserves local receptionist capacity for daily acute care requests.
- Parallel Outcome Tracking: Relying on secondary data logging alongside standard electronic health records ensures that specific clinical shifts (such as deprescribing or titrating) are instantly reportable to partners.
- Standardized Continuity via Handover Forms: Utilizing unified digital handovers ensures that whenever clinical pharmacists identify escalating risks, practice partners are informed through a consistent, predictable communication channel.
The Problem
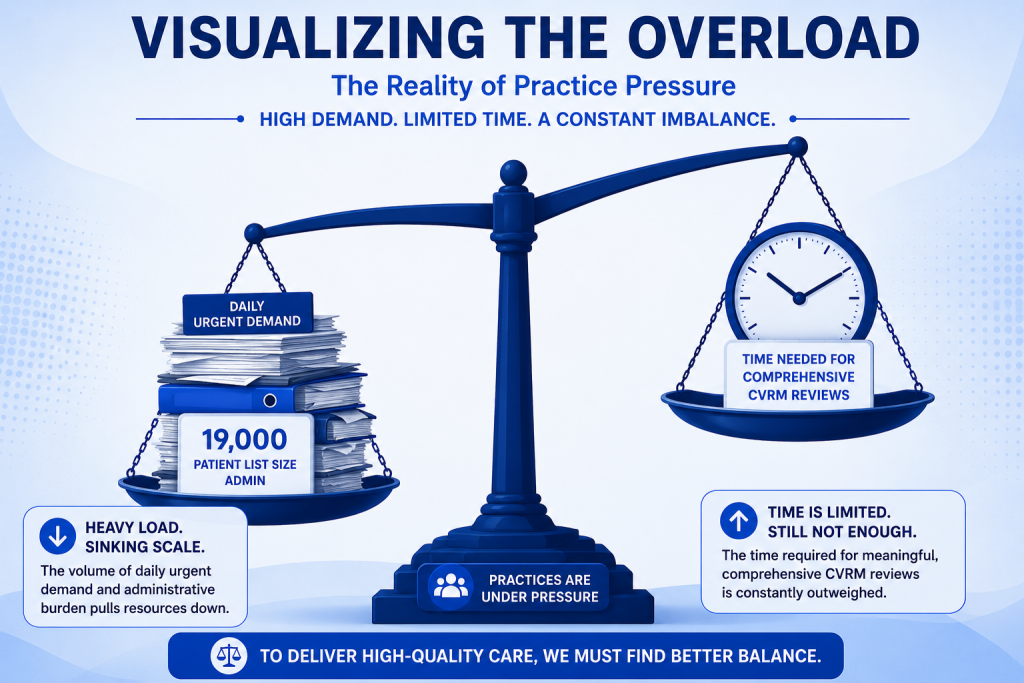
With an extensive patient registry of 19,000 individuals, Elm Tree Practice faced a compounding workload. National primary care frameworks demand structured, clinical reviews for complex, multi-morbid patients. However, when clinical teams are stretched thin by urgent on-the-day demand, these intensive reviews risk becoming rushed exercises designed merely to pass an audit.
The partners recognized that their vulnerable patient cohorts, particularly those requiring rigorous cardiovascular risk management primary care oversight, needed unhurried, evidence-based evaluations. Undertaking these detailed reviews internally meant diverting clinicians from standard clinics, creating an unsustainable imbalance in daily operations.
The Challenge
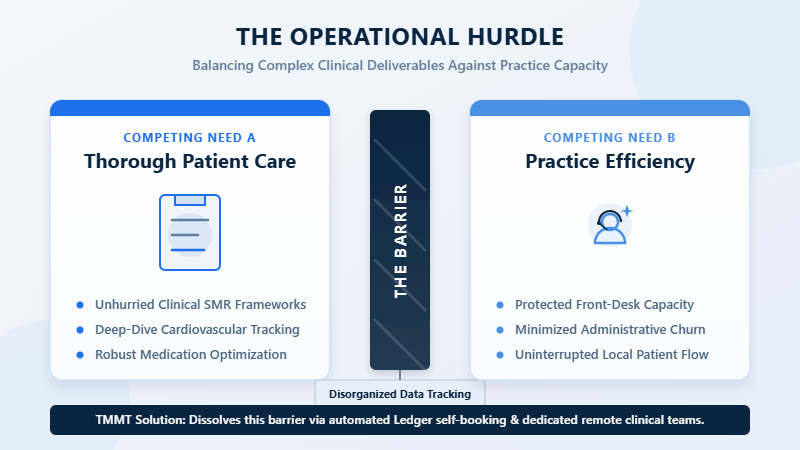
The primary operational hurdle was not just the delivery of clinical knowledge, but the significant administrative trailing work required to support it. A successful review campaign typically requires:
- Sifting through patient lists to identify specific qualifying medication profiles.
- Managing multiple outbound phone calls, handling patient rejections, and rescheduling missed appointments.
- Documenting nuanced data regarding which medications were started, stopped, reduced, or carefully titrated over time.
For Elm Tree Practice, the core challenge was clear: how to safely deploy an optimized clinical pharmacist workload to manage 114 highly complex patient files without creating a secondary wave of booking and tracking tasks for the practice’s existing administrative staff.
The Solution
The Medicines Management Team (TMMT) introduced an end-to-end operational framework that integrated directly into the practice’s ecosystem using national ARRS funding allocations. This approach removed the burden of execution from the local team entirely.
To eliminate booking administration, TMMT deployed a patient self-booking workflow via Ledger. The remote clinical team handled outbound contact seamlessly, resulting in zero failed calls. Clinically, the pharmacists did not merely log the reviews within the practice’s core medical software; they maintained a parallel Excel tracking structure. This documented exactly which medications were initiated, stopped, down-titrated, or adjusted, giving practice partners immediate visibility into the program’s clinical value. Daily communication was sustained through organized Microsoft Teams syncs and standardized Handover Forms.
Outcomes Achieved
The metrics compiled at the conclusion of the project demonstrate the direct, measurable value generated by shifting to a structured, dedicated model. Out of the 114 targeted patients, 109 comprehensive medication reviews were successfully finalized. The remaining balance consisted of only two patient declines and three individuals who remained non-contactable, representing a 100% service delivery rate across all reachable candidates.
The depth of these reviews is reflected in the high volume of medicines optimization impact metrics recorded:
- 171 Total Optimization Interventions: Moving far beyond basic box-ticking, the clinical team delivered 171 distinct actions directly enhancing safety and clinical effectiveness.
- 51 Medicines Safely Stopped/Deprescribed: Eliminating inappropriate polypharmacy and reducing the risk of adverse drug reactions.
- 57 Dose Optimization Interventions: Adjusting medication strengths to bring patients strictly in line with therapeutic targets.
- 63 Medication Monitoring Interventions: Ensuring appropriate laboratory follow-ups and safety tracking parameters were established.
Beyond these core therapeutic interventions, the team addressed systemic, long-term efficiency by configuring 104 electronic Repeat Dispensing (eRD) setups and executing 109 repeat synchronizations. Furthermore, the holistic nature of the reviews resulted in 109 lifestyle interventions logged and 28 targeted smoking cessation interventions initialized.

Conclusion
As primary care networks continue to scale, managing complex patient workflows requires highly structured, scalable solutions. This Structured Medication Reviews case study confirms that large practices do not have to compromise on clinical depth to meet administrative targets. By embedding an external, fully managed clinical framework, Elm Tree Practice achieved thorough cardiovascular risk management while completely shielding its internal staff from administrative strain.
The GP partners expressed high satisfaction with the precision and systemic impact of the recorded interventions. This project proves that with clear execution models, a busy practice can successfully transition regulatory compliance obligations into an opportunity for high-quality, proactive patient care.
To see how your primary care network can optimize its clinical capacity and streamline complex review workflows, visit the TMMT Medicines Management Service Page to discover our structured, remote support options.






